











Mexico’s Healthcare Reform

Sector research is one of the key directions of Galt & Taggart Research. We currently provide coverage of Energy, Tourism, Real Estate, Agriculture, and Wine sectors in Georgia. Healthcare is our latest addition, with the full report to be released in the near future. We are featuring two cases from the report for Georgia Today. Today’s article will provide an overview of Mexico’s healthcare reform and our next article will cover Turkey. These two countries have become global benchmarks for building universal healthcare (UHC) systems.
Every government in the world faces five major healthcare issues: aging population, chronic diseases, rising costs, quality of and access to healthcare, and insufficient infrastructure and technology. Mexico has been one of the global leaders in healthcare reform and has made a huge leap forward over the last few years with its UHC system - a healthcare system which provides access to healthcare for all citizens of a country.
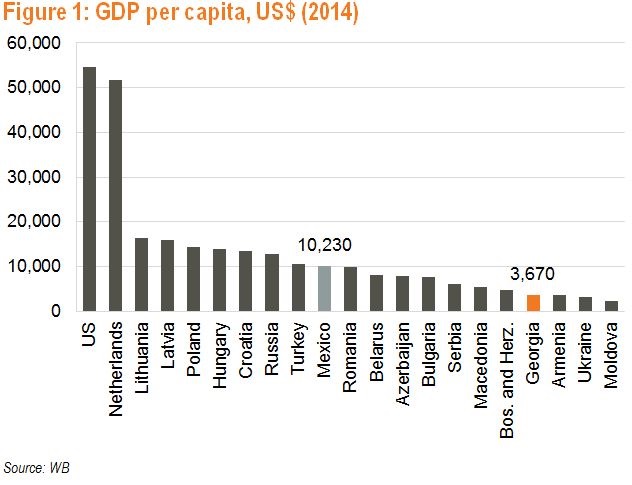
Economic disparity among the population is a problem in Mexico, despite having the world’s 15th largest economy (US$ 1.3tn as of 2014) and one of the highest GDP per capita in Latin America (US$ 10,230 as of 2014). In 2012, more than half of the 113mn population lived below the poverty line, compared with 9.7% of Georgia’s 4.5mn population.
In the early 2000s, half of the Mexican population was uninsured. Although the uninsured had access to services offered by public health facility networks, the distribution of public funds among population groups and states was inefficient and inequitable. The uninsured half of the population received only 1/3 of federal funding for health and there was a 5 to 1 difference in spending per capita across states in 2003. Every year, 2-4mn households (9-18% of all households) suffered from catastrophic healthcare payments. Public healthcare spending was below the Latin American average and was too low to address even the basic healthcare needs. Out-of-pocket spending accounted for more than half of healthcare spending in Mexico, above that of Brazil, Chile, and Colombia. The share of private spending was even larger in Georgia (4.6-5.7x that of public spending) and around 65.0% of medical care in Georgia was either self-treatment or provided free of charge from relatives or neighbourhood doctors.
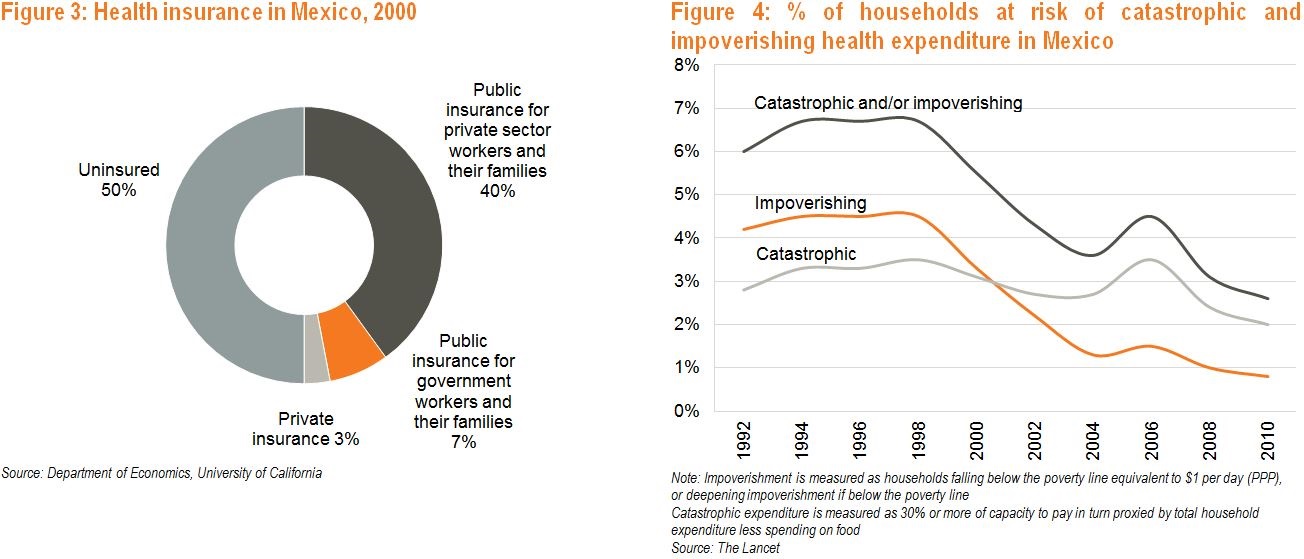
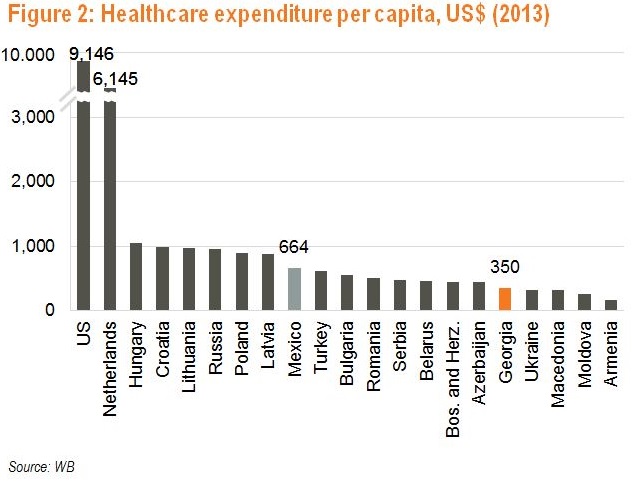
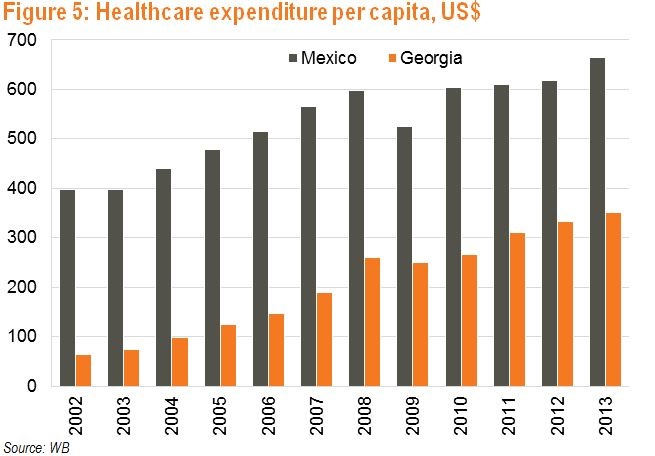
In response, in 2003 Mexico designed structural reforms to protect families from impoverishing health spending and to completely cover the country’s roughly 12mn uninsured families (about 55% of all households). Similar to Georgia, the main challenge for Mexico was the disparity in the allocation of healthcare financing as well as services among population groups and states. The Seguro Popular, the new publicly funded insurance plan, took over in 2004 (Georgia started its insurance reform in 2007) with the goal of achieving 100% coverage in 7 years (Georgia introduced it in 6 years). The program was implemented in stages, taking into account the states’ individual characteristics, and enrolment was first targeted at the poorest segment of the population. The Seguro Popular was financed by both state and federal governments as well as by beneficiary families. The federal government contributed a uniform amount for all families. Each enrolled state contributed an equal amount for every insured family and family-level contribution was determined by disposable income. From 2002 to 2013, Mexico’s healthcare spending per capita increased from US$ 396 to US$ 664. Over 2002-13, public health expenditure more than doubled from US$ 18.3bn to US$ 40.7bn.
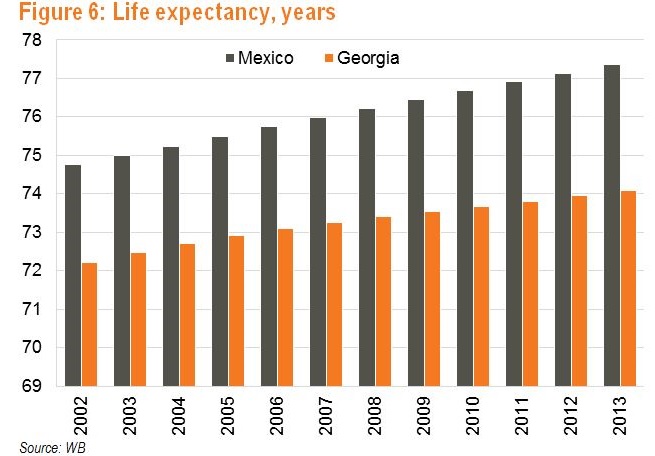
Due to improved access to and quality of care, life expectancy in Mexico increased over the last decade to 79.8 for females and 75.1 for males as of 2013, up from 77.2 and 72.3 in 2002, respectively. Mexico also improved its health resources and by 2013, it had 2.2 physicians and 2.6 nurses per 1,000 persons (compared to 1.5 and 2.2 in 2002, respectively). However, as of 2013, Mexico had the lowest number of hospital beds per 1,000 persons among OECD countries - 1.5 compared to an average of 5.0.
Despite these strides, Mexico’s public healthcare system faces considerable challenges, including insufficient infrastructure, poor distribution of resources among federal entities, and limited public-private partnerships for infrastructure development. There is also little focus on wellness and prevention - only 0.6% of budget disbursements for the health sector are used for the promotion of health and prevention and control of communicable and degenerative diseases and injury. The private healthcare system has challenges as well, including a deficit of nurses, since wages and benefits are lower than those offered by the public sector.
The inefficiency of the system was the main problem hindering the development of Mexico’s healthcare system. Mexico’s case shows that increased government funding, equality in funding allocation, proper timing, and efficient management were the key contributors to the turnaround of the country’s healthcare system.
David Ninikelashvili (Galt and Taggart)